Motilium
Samford University. O. Jens, MD: "Buy Motilium no RX - Effective Motilium".
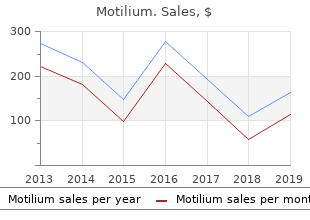
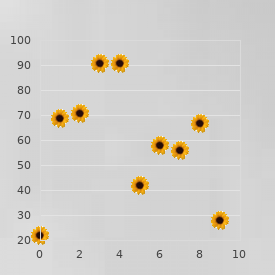
At the question mark order motilium online from canada gastritis diet on a budget, just before 1994 generic 10 mg motilium amex gastritis diet during pregnancy, the data can no longer resolve the trunk lineage because several variants cocirculated at thattimeandthetrunkcanberesolved only after one knows which of those lineages succeeded buy 10 mg motilium with amex gastritis quick cure. The filled circles show four isolates from 1994 that represented the four classifications for variable amino acids. Shd5 (A/Shangdong/5/94) represented the lineagewiththegreatest number of recent amino acid changes at sites that had been positively selected in the past, as inferred from the 1983–1997 data. The Har3 (A/Harbin/3/94) lineage had variant amino acids near the receptor binding site. The Sant (A/Santiago/7198/ 94) lineage had variant amino acids at those sites that had evolved rap- idly in the past. The NY15 (A/New York/15/94) lineage had variant sites in or near antibody epitopes A and B. Those data show which of the 1994 lineages succeeded and which died out. Suc- cessful prediction means choosing the isolate closest on the tree (most alike genetically) with the lineagethatcontinues along the trunk and gives rise to the future population. It turned out that Shd5 was closest to the successful trunk lineage among the candidates. In other words, the most changes in previously positively selected sites predicted which lineage succeeded in subsequent years. In nine of those elevenyears,thelineage that contained the most changes relative to its ancestor at the eighteen positively se- lected sites identified the section of the tree from which the future trunk emerged. The sites in the antibody epitopes only identified seven of eleven trunk lineages, and the other amino acid sets did worse. Thus, positive selection provided the best signal for which amino acid changes correlated most closely with fitness. The epidemic strains con- tained amino acid replacements at a small number of sites that had previously been identified as crucial for escape from monoclonal anti- bodies. It would be interesting to compare these two methods in a single study of the same evolving parasite population. Substitutions at these positively selected sites correlated with the future success of MEASURING SELECTION 261 lineages during the years of sampling, 1983–1997. In the future, will these eighteen sites continue to be the primary target of selection? On the one hand, the eighteen sites may indeed be the most important for escape from protective antibodies. Ifso,futuresamples will continue to find positive selection focused onthesesites. On the other hand, different sites may dominate in the future, with little future selective change in the currently positively selected sites. A changing focus of selection may arise from evolving structural features of the viral surface that expose or hide different sites or from a changed distribution in the immune memory profiles of hosts. If episodic selection frequently occurs, then the time scale over which one studies substitution patterns plays a critical role in inference. Sim- ply measuring aggregate rates of synonymous and nonsynonymous sub- stitutions may turn out to be a rather crude tool that misses a large proportion of the changes brought about by natural selection. As more data accumulate, it will become important to match statistical methods with explicit hypotheses about the biological processes of selection and the temporal scale over which selection varies.
Diseases
- Carcinoma of the vocal tract
- PEHO syndrome
- Ambral syndrome
- Dermatomyositis
- Byssinosis
- Floaters
In addition purchase motilium overnight gastritis diet �������, most studies evaluated health outcomes such as quality of life cheap motilium 10 mg amex gastritis diet ������, functional capacity (e buy cheap motilium 10 mg line gastritis and celiac diet. Various observational studies enrolled primary care patients who started on targeted immune modulator treatment. Because these studies included unselected populations, findings were probably more applicable to the average rheumatoid arthritis patient than results from efficacy trials. Limitations with respect to risk of bias have to be kept in mind though. Sponsorship All trials were funded by the pharmaceutical industry. Meta-analyses and cohort studies usually had public or a mix of public and industry funding. Detailed assessment: Direct evidence on comparative effectiveness Overall, we included eight head-to-head studies comparing one targeted immune modulator to 39-45,48 another. These direct comparisons, however, were limited to abatacept compared with infliximab, adalimumab and etanercept compared with infliximab, and adalimumab compared Targeted immune modulators 29 of 195 Final Update 3 Report Drug Effectiveness Review Project with etanercept. We could not find any head-to-head evidence for any of the other drugs. Abatacept compared with infliximab The only double-blinded head-to-head trial, the ATTEST (Abatacept or infliximab compared with placebo, a Trial for Tolerability, Efficacy, and Safety in Treating rheumatoid arthritis) 39 study, was a fair randomized controlled trial that compared abatacept with infliximab. This study enrolled 431 patients and randomized them to abatacept (10 mg/kg every 4 weeks + methotrexate), infliximab (3 mg/kg every 8 weeks + methotrexate), or placebo. The primary outcome was assessed at 6 months followed by a double-blinded extension phase up to 1 year. No statistically significant differences in efficacy were obvious between treatments at 6 months (DAS 28: abatacept ‒2. At 1 year, however, significantly more patients on abatacept than on infliximab achieved American College of Rheumatology 20 response (American College of Rheumatology 20 response 72. Likewise, health-related quality of life measures (Health Assessment Questionnaire Disability Index, Short Form 36 Health Survey) improved statistically significantly more with abatacept than with infliximab treatment. It has to be noted though, that infliximab was administered at a fixed dose regimen throughout the entire study. Infliximab efficacy trials have shown that up to 30% of patients require dose increases. Adalimumab compared with etanercept The evidence on the comparative effectiveness of adalimumab and etanercept is limited to a 44 45 good and a fair observational study. Both studies were based on national registers of targeted immune modulators (the Danish DANBIO [Danish Biological] and the Dutch DREAM [Dutch Rheumatoid Arthritis Monitoring]) and were conducted prospectively in primary care based populations. Both studies enrolled patients who had failed at least one conventional disease- modifying antirheumatic drug and were started on a targeted immune modulator. The choice of the treatment and dosing was at the discretion of the treating rheumatologist. Overall, 356 44 patients were followed up for 12 months in the study based on the DREAM register, and 969 45 patients in the study based on the DANBIO register. After 12 months of follow-up, treatment responses in both studies were similar for patients on adalimumab and etanercept. The primary outcome of the DREAM study was the 44 DAS28 course over a 12 months follow-up, as analyzed on an intent-to-treat basis.
Diseases
- Rickettsiosis
- Winchester syndrome
- Optic disc drusen
- Ota Kawamura Ito syndrome
- Lamellar recessive ichthyosis
- Organic personality syndrome
- Aberrant subclavian artery
- Brachymetapody anodontia hypotrichosis albinoidism
- Dandy Walker malformation with mental retardation, macrocephaly, myopia, and brachytelephalangy
Newer drugs such as pritelivir buy generic motilium pills gastritis symptoms treatment mayo clinic, that do not inhibit DNA polymerase but rather heli- case order motilium with a visa gastritis and nausea, another herpes virus enzyme discount 10 mg motilium with amex gastritis diet �������������, have been effective in clinical trials (Tyring 2011, Wald 2014). However, additional studies are warranted to define the potential of helicase inhibitors. A local anesthetic that can be produced by the pharmacist can be prescribed in addi- tion for painful mucocutaneous lesions. Unfortunately, the approved tetracaine solu- tion (HervirosTM) has been taken off the market. Some pharmacists can, however, confect something similar in-house. However, a meta-analysis of almost 2000 patients in eight randomized studies showed that acyclovir can reduce the risk of both HSV and HZV disease by more than 70%. The introduction of ART has changed the relevance of this data. Nevertheless, it can still make sense, even today, to treat persistent recurrences with long-term low-dose acyclovir or valacyclovir (DeJesus 2003, Warren 2004). However, short bursts of subclinical genital HSV reactivation are frequent, even during high- dose acyclovir therapy (Johnston 2012). Herpes simplex vaccines are still in early stages of development (Belshe 2012). Treatment/prophylaxis of HSV infection (daily doses) Acute therapy Duration: 7–14 days Treatment of choice Acyclovir Acyclovir 1 tab. Large randomized studies demonstrated that during anti-HSV therapy, HIV replication is also inhibited. During treatment with acyclovir, HIV plasma viremia is decreased by 0. High dose valacyclovir resulted in a slightly greater reduction of HIV replication (Mugwanya 2011, Perti 2013). Even the rate of disease progression can be reduced. In a large randomized trial in Uganda, acyclovir showed a significant clinical benefit, with the greatest effect in individuals with a high baseline viral load (Reynolds 2012). Despite the fact that acyclovir does not prevent the transmission of HIV (Celum 2008+2010, Watson-Jones 2008), these results have recently revived the interest in acyclovir therapy (Vanpouille 2009). Possibly new derivatives will be developed that are better tolerated and more effec- tive in terms of HIV antiviral potency. Efficacy results of a trial of a herpes simplex vaccine. Effect of aciclovir on HIV-1 acquisition in herpes simplex virus 2 seropositive women and men who have sex with men: a randomised, double-blind, placebo-controlled trial. Acyclovir and transmission of HIV-1 from persons infected with HIV-1 and HSV-2. A comparison of topical application of penciclovir 1% cream with acyclovir 3% cream for treatment of genital herpes: a randomized, double-blind, multicentre trial. Valaciclovir versus aciclovir for herpes simplex virus infection in HIV-infected individuals: two randomized trials. Valacyclovir for the suppression of recurrent genital herpes in HIV-infected subjects. Freeman EE, Weiss HA, Glynn JR, Cross PL, Whitworth JA, Hayes RJ. Herpes simplex virus 2 infection increases HIV acquisition in men and women: systematic review and meta-analysis of longitudinal studies. Clinical efficacy of high-dose acyclovir in patients with HIV infection: a meta-analysis of randomized individual patient data.